
7 Sample EMS Narrative Formats to Master in 2025
Effective documentation is the cornerstone of great patient care and sound operations. A well-written patient care report (PCR) not only ensures continuity of care but also provides critical legal protection and is essential for accurate billing and reimbursement. However, many EMS professionals fall into a routine, using the same narrative style for every call, which can lead to incomplete records and significant lost revenue. This guide moves beyond the basics to explore seven distinct types of EMS narratives, providing a detailed sample EMS narrative for each specific scenario.
We'll break down the structure of each format, from SOAP to Mechanism-Based Trauma, offering practical examples and actionable insights. You'll learn not just how to write them, but strategically when to use each format to maximize clarity, efficiency, and your agency's financial health. Properly documenting every billable action, like IV starts or cardiac monitoring, is key to fiscal stability. For example, failing to document a second IV attempt still represents a billable supply used; precise documentation captures this cost. To truly elevate your patient care reports, it's crucial to understand and apply professional writing standards, ensuring your narratives are clear, impactful, and defensible. For a deeper dive into this, consider these guidelines on mastering professional writing standards to further refine your skills. Let’s examine the samples.
1. SOAP Method EMS Narrative
The SOAP method is a foundational structure for clinical documentation and a cornerstone of effective EMS narratives. It provides a logical, organized framework that ensures all critical patient information is captured and communicated clearly. This method divides the patient care report into four distinct sections, guiding the provider from initial patient contact to the final treatment plan.
The SOAP acronym stands for:
- S – Subjective: This section captures the patient's story. It includes their chief complaint, history of present illness, and any relevant past medical history, all from the patient's (or a bystander's) perspective. Using direct quotes like, "My chest feels like an elephant is sitting on it," can be incredibly powerful here.
- O – Objective: Here, you document your unbiased, measurable findings. This includes vital signs (blood pressure, pulse, respirations), physical exam results, and diagnostic data like blood glucose levels or EKG interpretations. Crucially, this section should also include pertinent negative findings, such as "no JVD" or "equal and bilateral breath sounds."
- A – Assessment: This is your clinical impression or field diagnosis based on the subjective and objective data. It's where you synthesize the information to form a professional judgment, such as "Acute Coronary Syndrome" or "Hypoglycemic Emergency."
- P – Plan: This final section details the actions you took. It outlines every intervention, from administering oxygen and medications to splinting a fracture, and documents the patient's response to each treatment. For example, detailing "12-lead EKG acquired and transmitted" is not just good patient care, it's a billable procedure that must be documented to be reimbursed, saving the agency from losing hundreds of dollars per call.
The SOAP Narrative Flow
This timeline infographic illustrates the logical progression of information when constructing a SOAP-based sample ems narrative.
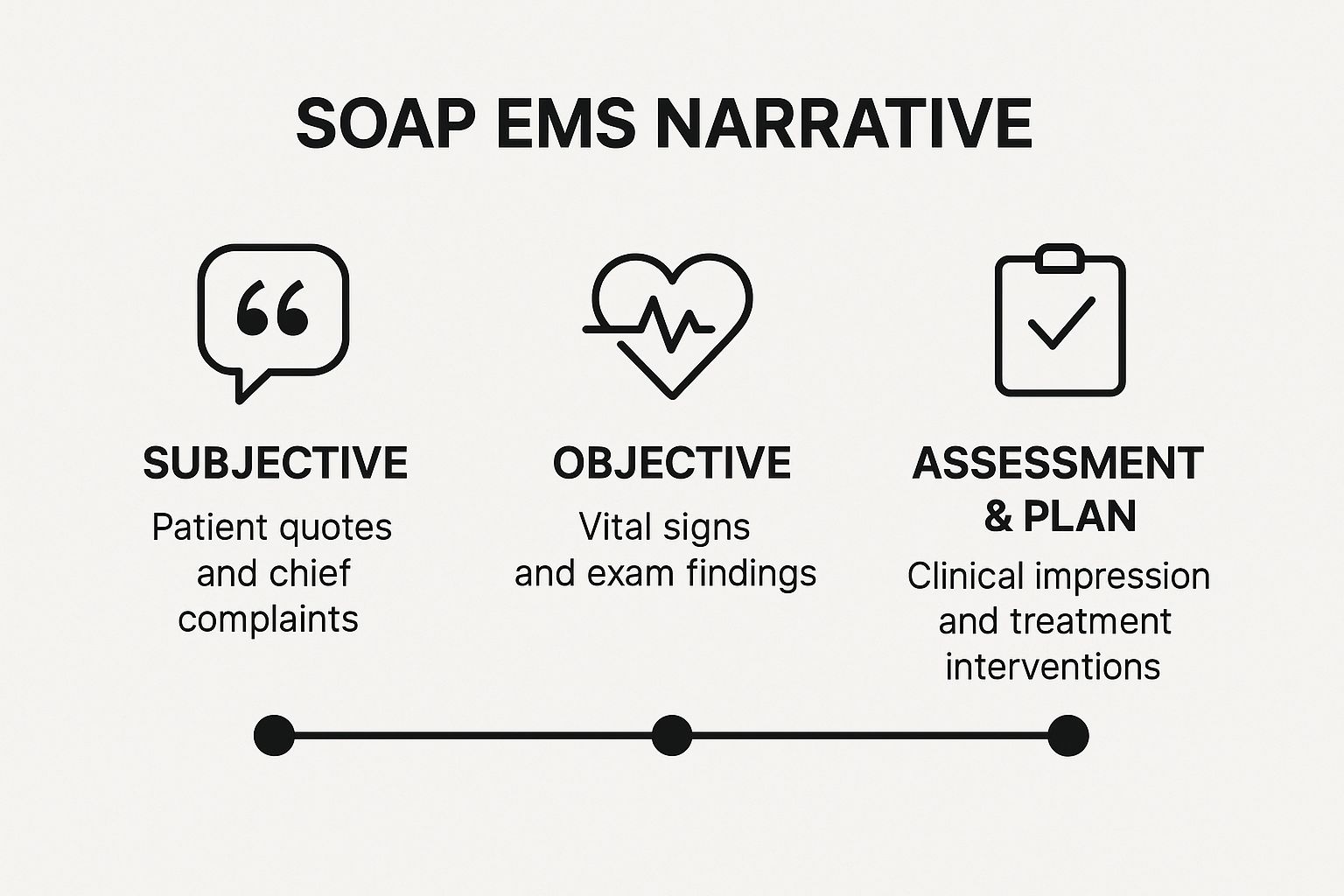
The visualization shows how each step builds upon the last, moving from the patient's personal account to objective data and finally to the provider's clinical judgment and actions. A practical example for an asthma patient might be:
- S: Pt states "I can't catch my breath," history of asthma, used inhaler x2 without relief.
- O: Vitals: HR 120, RR 28, SpO2 91%. Wheezing noted in all lung fields.
- A: Acute Asthmatic Exacerbation.
- P: O2 via NRB at 15LPM, Albuterol/Ipratropium nebulizer administered. Reassessment showed decreased wheezing, RR 22, SpO2 96%. Transported to St. Francis ED.
Why This Method Works
The SOAP format is widely adopted by major systems like FDNY EMS because it creates a defensible, chronological record that is easily understood by other healthcare providers. For those looking to streamline their SOAP Method EMS Narrative, exploring various options for utilizing a dedicated template can be highly beneficial. Many high-quality free SOAP note templates are available to help ensure consistency and completeness, which can reduce documentation time and minimize the risk of billing errors or legal challenges.
2. Chronological EMS Narrative
The Chronological EMS Narrative documents events precisely in the order they occurred, from the initial dispatch to the final patient transfer at the receiving facility. This method creates a clear, timeline-based account that vividly illustrates the sequence of assessments, interventions, and any changes in the patient's condition throughout the duration of the call.

Unlike other formats that group information by type, the chronological approach focuses on the "when." It's particularly effective for complex calls where the timing of events is critical to understanding the patient's clinical course. A practical example for a cardiac arrest would include precise timestamps:
- 14:02: Dispatched to unresponsive male.
- 14:08: Arrived on scene. Found male, approx. 60s, apneic and pulseless.
- 14:09: CPR initiated. AED applied, analyzed, shock advised.
- 14:10: 1st shock delivered. CPR resumed.
- 14:12: IV established. 1mg Epinephrine administered.
- 14:15: ROSC achieved. Pt has palpable carotid pulse at 70 bpm.
The Chronological Narrative Flow
This method follows a linear progression, using time as the primary organizing principle. A strong sample ems narrative using this format will clearly state what happened and when, leaving little room for ambiguity.
The video provides practical insights into structuring a narrative that logically presents the flow of a call, which is the core strength of the chronological method.
Why This Method Works
A chronological narrative creates an irrefutable legal and medical record. By time-stamping key events, you provide a clear justification for your clinical decisions at each step. This precision is invaluable for quality assurance reviews, legal proceedings, and continuity of care. Using this format correctly can significantly reduce billing rejections caused by unclear or incomplete timelines. For example, documenting the exact time CPR was started and for how long directly supports billing for life support services, preventing a costly down-coding of the claim. This saves an agency money by ensuring prompt and full reimbursement.
3. Body Systems Assessment EMS Narrative
The Body Systems Assessment method structures a narrative around a systematic review of the body's major physiological systems. This approach provides a meticulous and comprehensive overview of the patient's condition, making it exceptionally useful for complex medical calls, interfacility transfers, and any situation requiring a detailed physical examination. It organizes findings logically by system, such as cardiovascular, respiratory, and neurological.
This methodical documentation ensures no critical detail is overlooked. By systematically addressing each body system, providers create a thorough clinical picture that is easy for receiving facility staff to interpret. This comprehensive approach is particularly valuable for painting a complete patient status, justifying treatment decisions, and ensuring continuity of care.

This sample ems narrative structure is based on a head-to-toe assessment, broken down by anatomical and physiological systems. Here’s a practical example for a patient with sepsis:
- Neurological: A&O x2, confused. GCS 13. Pupils equal and reactive.
- Cardiovascular: Tachycardic at 130 bpm, BP 88/50. Skin is pale, cool, and diaphoretic.
- Respiratory: RR 26 and shallow. Lungs clear but with diminished sounds in bases. SpO2 93% on room air.
- Gastrointestinal/Genitourinary (GI/GU): Abdomen soft, non-tender. Pt reports decreased urine output today.
- Integumentary: Skin is warm and flushed, no rashes noted.
- Musculoskeletal: Moves all extremities with generalized weakness. No edema.
Why This Method Works
The Body Systems Assessment narrative excels in cases with multiple comorbidities or unclear etiologies, providing a structured way to document a vast amount of information. This detailed record is legally robust and significantly improves the quality of the handoff report. For EMS agencies, a well-documented assessment can streamline the billing process. For instance, clearly noting findings across multiple systems substantiates the medical necessity for Advanced Life Support (ALS) level of care, preventing insurers from down-coding the service to a lower-paying BLS level. This defensible report can prevent costly audits and save thousands in potential revenue loss.
4. CHART Method EMS Narrative
The CHART method offers another highly structured alternative for crafting a clear and concise EMS narrative. It streamlines the documentation process by focusing on the chronological flow of the patient encounter, from the initial complaint to the final disposition. This method is particularly effective for straightforward calls where a linear progression of events needs to be documented efficiently.
The CHART acronym stands for:
- C – Chief Complaint: This section starts with the patient's primary reason for calling EMS, ideally in their own words. It sets the scene for the entire report.
- H – History: Here, you document the history of the present illness (HPI) using frameworks like OPQRST, as well as relevant past medical history, medications, and allergies. The key is to include only the history pertinent to the chief complaint.
- A – Assessment: This is where your objective findings are recorded. It includes the primary and secondary physical assessments, vital signs, and any diagnostic results like a blood glucose level or EKG findings.
- R – Rx/Treatment: "Rx" is shorthand for treatment. This section details all interventions performed, including medications administered, procedures like splinting or bleeding control, and the patient's response to these treatments.
- T – Transport: This final part documents the details of the transport, including the patient's position, their status during transport (e.g., stable, deteriorating), and any changes noted en route to the receiving facility.
The CHART Narrative Flow
The CHART method is especially useful for Basic Life Support (BLS) calls. A practical example for a simple fall:
- C: 82-year-old female c/o left hip pain.
- H: Pt states she slipped on a rug. Denies LOC. Hx of osteoporosis.
- A: Vitals stable. Obvious deformity and shortening to left leg. Pedal pulse intact.
- R: Pt placed on backboard, left leg splinted in position found. Pain managed with ice pack.
- T: Transported non-emergent to Memorial Hospital. Pt remained stable.
By moving from complaint to history, assessment, treatment, and finally transport, the narrative naturally tells the complete story of the call. This logical progression is vital for creating a comprehensive and defensible sample ems narrative.
Why This Method Works
CHART provides a simple yet comprehensive framework that ensures all critical aspects of patient care are documented. Its linear structure makes it easy for other healthcare providers, quality assurance officers, and billing departments to follow the sequence of events. For agencies, adopting a standardized method like CHART can significantly improve consistency. This standardization directly impacts billing accuracy and reduces claim denials by ensuring all elements of care are captured. For example, explicitly documenting treatment (Rx) and transport details (T) prevents claims from being rejected for lack of information, saving money by minimizing administrative rework.
5. Problem-Oriented EMS Narrative
The problem-oriented method organizes documentation around specific patient problems, which is ideal for complex cases with multiple complaints. Instead of a single, linear story, this approach creates mini-narratives for each issue, ensuring that no detail is overlooked. This is particularly effective for geriatric patients with comorbidities or multi-system trauma victims.
This method requires the provider to:
- Identify Problems: Systematically list each patient complaint or clinical problem discovered during the assessment. This could range from "chest pain" and "shortness of breath" to "left ankle deformity."
- Assess Each Problem: For every identified problem, document the relevant subjective and objective findings. This creates a focused assessment for each specific issue.
- Plan for Each Problem: Detail the interventions and treatments provided for each problem individually. This clearly links your actions to specific patient needs.
- Update and Reassess: Continuously update the problem list as new issues arise or existing ones resolve during patient care.
The Problem-Oriented Narrative Flow
This approach excels in situations where a single narrative would become convoluted. Consider an elderly patient who fell: they may present with a hip fracture, a head laceration, and an underlying cardiac issue that caused the fall. A problem-oriented sample ems narrative would create a numbered list:
- Problem: Left Hip Pain. Assessment: Deformity, shortening. Plan: Splint, monitor distal pulses.
- Problem: Head Laceration. Assessment: 3cm lac to forehead, active bleeding controlled. Plan: Apply pressure dressing.
- Problem: Syncope. Assessment: Pt reports dizziness prior to fall. EKG shows Atrial Fibrillation at 130. Plan: IV access established, cardiac monitoring.
This organized structure prevents critical information from getting lost and demonstrates a comprehensive, systematic approach to patient care.
Why This Method Works
The problem-oriented narrative is highly valued in complex medical scenarios because it enhances clarity and thoroughness. It forces providers to think critically about each patient issue. This meticulous approach directly supports accurate billing by clearly justifying each intervention. For instance, documenting a splint for "Problem 1: Ankle Fracture" and cardiac monitoring for "Problem 2: Atrial Fibrillation" leaves no ambiguity for billing coders. This prevents an insurer from denying the cardiac monitoring charge on a trauma call. This precision minimizes claim rejections and ensures proper reimbursement, saving the agency time and money.
6. Mechanism-Based Trauma EMS Narrative
The Mechanism-Based Trauma narrative is a specialized format designed for calls involving physical injury. It prioritizes a detailed account of the scene and the forces involved, known as the mechanism of injury (MOI), to create a clear picture of potential injuries before they are even clinically apparent. This approach helps the receiving hospital's trauma team anticipate patient needs and mobilize resources effectively.

This narrative structure is built around the following core components:
- Scene Description: This section paints a vivid picture of the environment. For a motor vehicle accident, this includes details like the extent of vehicle damage ("significant frontal intrusion"), road conditions, and the patient's position within the vehicle.
- Mechanism of Injury (MOI): Here, you document the specific forces that likely caused the injuries. This involves describing the kinematics, such as "unrestrained driver in a high-speed, head-on collision" or "fall from approximately 20 feet onto a concrete surface."
- Systematic Assessment: This details your head-to-toe trauma assessment, documenting injuries found and pertinent negatives. The findings should correlate directly with the MOI, linking the story of the event to the patient's physical condition.
- Interventions and Transport: This part outlines all trauma care provided, from cervical spine immobilization and hemorrhage control to establishing IV access and the decision for rapid transport to a designated trauma center.
The Mechanism-Based Narrative Flow
A strong mechanism-based trauma sample ems narrative follows a logical sequence that connects the event to the patient's injuries. A practical example:
Scene: Single vehicle MVC, moderate front-end damage with airbag deployment.
MOI: Restrained driver complains of chest pain after striking the steering wheel.
Assessment: Pt alert, vitals stable. Large hematoma to anterior chest wall. Breath sounds equal. Denies head/neck/back pain.
Interventions: C-collar applied for precaution, 12-lead EKG shows sinus tach. IV established. Rapid transport to trauma center initiated due to high index of suspicion for cardiac contusion.
This foresight can be critical in identifying occult injuries and improving patient outcomes.
Why This Method Works
This method is crucial for trauma care because it emphasizes the "index of suspicion." By thoroughly documenting the MOI, you provide the rationale for your treatment decisions and help the receiving facility prepare for the worst-case scenario. This level of detail is essential for both clinical handoff and legal protection. A well-documented MOI can justify activating a trauma team, which avoids unnecessary costs for the hospital and patient if a full activation isn't warranted. For the agency, it justifies a higher level of care and transport destination, ensuring proper billing and preventing revenue loss from under-triage.
7. Focused Assessment EMS Narrative
The focused assessment narrative is a highly efficient documentation method that concentrates on the specific body system or area directly relevant to the patient's chief complaint. This streamlined approach allows for detailed documentation of pertinent findings while avoiding unnecessary information, making it ideal for clear-cut, single-system issues.
This method is particularly effective for calls where the problem is well-defined and isolated. By narrowing the scope, the provider can create a clear, concise, and clinically relevant report that paints a vivid picture of the specific issue without getting bogged down in extraneous details.
The core principles of this narrative style are:
- Specificity: The narrative hones in on the affected area or system. For an isolated extremity injury, the focus is on the limb's neurovascular status, range of motion, and physical signs of trauma.
- Pertinence: Only information that contributes to understanding the chief complaint is included. This includes both positive and negative findings within the focused system.
- Justification: The narrative should implicitly or explicitly justify why a limited assessment was appropriate, often by stating the patient denies other complaints or symptoms.
- Efficiency: This approach saves time on scene and during documentation, allowing for quicker report completion. This efficiency translates directly into cost savings by reducing administrative hours and potential billing delays. Less time spent on paperwork means crews are available for the next call sooner, improving unit hour utilization and saving on overtime costs.
The Focused Narrative Flow
This sample ems narrative for a patient with an ankle injury demonstrates the focused assessment approach.
Chief Complaint: "I twisted my ankle and heard a pop."
Focused Assessment: "Patient is A&O x4, pleasant, and in no acute distress. Airway is patent, breathing is non-labored. Examination is focused on the left lower extremity. Obvious deformity and swelling noted to the lateral malleolus of the left ankle. Pedal pulse is strong and equal to the right. Capillary refill is less than 2 seconds. Patient is able to wiggle toes but reports significant pain with any movement of the ankle. Sensation is intact to light touch. The remainder of the physical exam is deferred as patient denies any other injuries or complaints."
This example zeroes in on the injury, providing a detailed yet brief account of the essential clinical findings.
Why This Method Works
A focused assessment narrative is highly defensible and clinically sound for specific call types like isolated extremity injuries or simple medical complaints. It demonstrates targeted, appropriate care and avoids charting by exception, which can be vague. This clarity and conciseness significantly reduce the likelihood of billing rejections or insurance queries, ensuring faster reimbursement and a healthier revenue cycle. By eliminating redundant information, it also saves valuable provider time, allowing crews to return to service more quickly.
7 EMS Narrative Methods Compared
| Narrative Method | Implementation Complexity 🔄 | Resource Requirements ⚡ | Expected Outcomes 📊 | Ideal Use Cases 💡 | Key Advantages ⭐ |
|---|---|---|---|---|---|
| SOAP Method EMS Narrative | Moderate – structured four-part format | Moderate – requires careful sectioning | Comprehensive, clear separation of subjective & objective data | General EMS documentation, training, healthcare systems | Widely recognized, easy to learn, comprehensive |
| Chronological EMS Narrative | Moderate to high – time-sequential detail | Moderate to high – needs accurate timestamps | Clear timeline showing event progression | Complex calls, multi-provider responses, trauma | Natural storytelling, cause-effect clarity |
| Body Systems Assessment EMS Narrative | High – detailed by body system | High – requires in-depth medical knowledge | Thorough and systematic patient evaluation | Medical transports, complex medical/trauma calls | Comprehensive, reduces missed findings |
| CHART Method EMS Narrative | Low to moderate – 5 focused components | Low – concise documentation | Concise yet complete clinical picture | Basic life support, routine transports, training | Easy to remember, balanced detail and brevity |
| Problem-Oriented EMS Narrative | High – problem-based with multiple plans | High – clinical skill needed | Clear problem identification, organized reasoning | Multi-complaint, complex chronic or psychiatric patients | Organized for multiple issues, shows clinical reasoning |
| Mechanism-Based Trauma EMS Narrative | High – trauma-focused with injury details | High – trauma expertise and detail | Detailed trauma assessment linked to injury mechanism | Trauma calls (MVC, falls, penetrating injuries) | Comprehensive trauma doc, assists hospital prep |
| Focused Assessment EMS Narrative | Low to moderate – focuses on chief complaint | Low – targeted and efficient | Efficient, complaint-specific documentation | Isolated complaints, stable patients, resource-limited | Time-efficient, reduces documentation burden |
Choosing the Right Narrative to Save Time and Money
Throughout this guide, we have explored seven distinct and powerful formats for crafting a sample ems narrative. From the structured logic of the SOAP and CHART methods to the targeted precision of a Focused Assessment or Mechanism-Based Trauma report, each style offers a unique lens through which to document a patient encounter. The goal is not to master just one, but to build a versatile toolkit that allows you to select the optimal format for any given situation, whether it's a routine medical call or a complex multi-system trauma.
Moving beyond a rigid, one-size-fits-all documentation strategy is the first step toward operational excellence. The most effective narrative is the one that tells the patient’s story with the greatest clarity, accuracy, and efficiency. This strategic choice has profound implications that extend far beyond the patient care report itself.
The Financial Impact of a Well-Crafted Narrative
A meticulously crafted narrative is one of your organization's most critical financial assets. Each report you write serves as the primary justification for billing and reimbursement. When a sample ems narrative clearly and comprehensively documents medical necessity, lists all procedures performed, and justifies the level of transport, it creates an ironclad record that drastically reduces the likelihood of insurance claim denials.
Consider the downstream costs of a poorly written report:
- Increased Administrative Overhead: Vague or incomplete narratives require hours of follow-up from billing staff to clarify details, leading to wasted time and increased labor costs.
- Delayed Reimbursements: Claim denials or requests for more information disrupt your revenue cycle, creating cash flow problems that can strain operational budgets.
- Legal and Compliance Risks: Inadequate documentation can become a significant liability during audits or legal challenges, potentially leading to costly fines or settlements.
By investing a few extra minutes on scene or immediately after a call to select and execute the right narrative format, you are making a direct investment in the financial health and stability of your service. It's a proactive measure that saves significant time and money on the back end.
Actionable Next Steps for Your Team
To translate these concepts into practice, focus on implementation. Begin by reviewing the narrative styles discussed in this article with your team. Hold brief training sessions to workshop different call scenarios, challenging your crew to identify the most efficient documentation method for each. Encourage providers to articulate why they chose a particular format, reinforcing the critical thinking behind the documentation.
An actionable insight is to create a simple cheat-sheet for the ambulance with call types and suggested narrative formats (e.g., MVC -> Mechanism-Based; Seizure -> Chronological; Diabetic -> SOAP). This small change can save crews mental energy and improve report consistency, directly reducing billing errors and saving money. The ultimate goal is to make narrative selection an intuitive part of every call. When your team can seamlessly pivot from a Chronological narrative for a complex timeline to a Body Systems approach for a detailed medical assessment, you not only improve patient handoffs but also fortify your agency's entire operational and billing process.
Ready to streamline your documentation and dispatch processes into a single, powerful platform? Discover how Resgrid, LLC can help your team manage calls, personnel, and reporting with ease, ensuring your narratives are as efficient as your response. Visit us at Resgrid, LLC to learn more.